















 1016 1030
1016 1030

2.1.7.
Pyelolithotomy
Once the pelvis is mobilized, the robotic ultrasound probe is utilized to
identify and confirm the location of the stone, and plan the incision
( Fig. 1 A). A vertical incision is made in the pelvis, until the stone is
exposed
( Fig. 1B). A robotic ProGrasp forcep is then used to carefully
dislodge and remove the stone/s
( Fig. 1C).
2.1.8.
Nephrolithotomy
The perinephric fat is cleared off the parenchyma overlying the location
of the stone. Scanning with the robotic probe identifies the stone with
presence of acoustic shadowing
( Fig. 2A). The incision line is planned in
the part of the parenchyma which is the thinnest. A linear nephrotomy
incision directly over the stone is thenmade using the robotic monopolar
hook
( Fig. 2B). This is done without clamping the renal hilum, and if
performed correctly, minimal bleeding is encountered. The stone is then
removed using the Prograsp as a single piece without fragmentation
( Fig. 2 C). In case the cavity containing the stone is thought to be in a
diverticulum, it is then ablated using argon beam or cautery.
2.1.9.
Flexible nephroscopy
After removing the stone, the ultrasound probe is redeployed to assess
for further stone(s) in the collecting system. If a stone is noted, and
inaccessible via the robotic instruments, a flexible nephroscope can be
inserted through an assistant port and manipulated into the renal pelvis
for inspection of the collecting system
( Fig. 3). This can be navigated by
the bedside assistant with guidance from the console surgeon. If a stone
is identified on nephroscopy, it is removed using a basket.
2.1.10.
Stent placement
During pyelolithotomy, a ureteral stent is placed. A 14-gauge Angiocath
needle is inserted by the bedside assistant and visualized by the robotic
surgeon. The assistant passes a guidewire through the catheter, which is
passed antegrade down the ureter. A double pigtail ureteral stent is then
inserted over the wire and advanced in the ureter with the aid of a pusher
until the mark on the stent indicates the proximal curl. The wire is then
withdrawn and the proximal curl placed into the renal pelvis.
2.1.11.
Closure
The pyelotomy is closed using a running 3-0 absorbable suture. For
nephrolithotomy, the incised renal parenchyma is closed using sliding
clip renorrhaphy technique with 1-0 vicryl absorbable sutures.
Hemostatic agents may also be applied over the defect. At the end of
the operation, the stone specimen is placed in an Endocatch bag and
retrieved through the camera port.
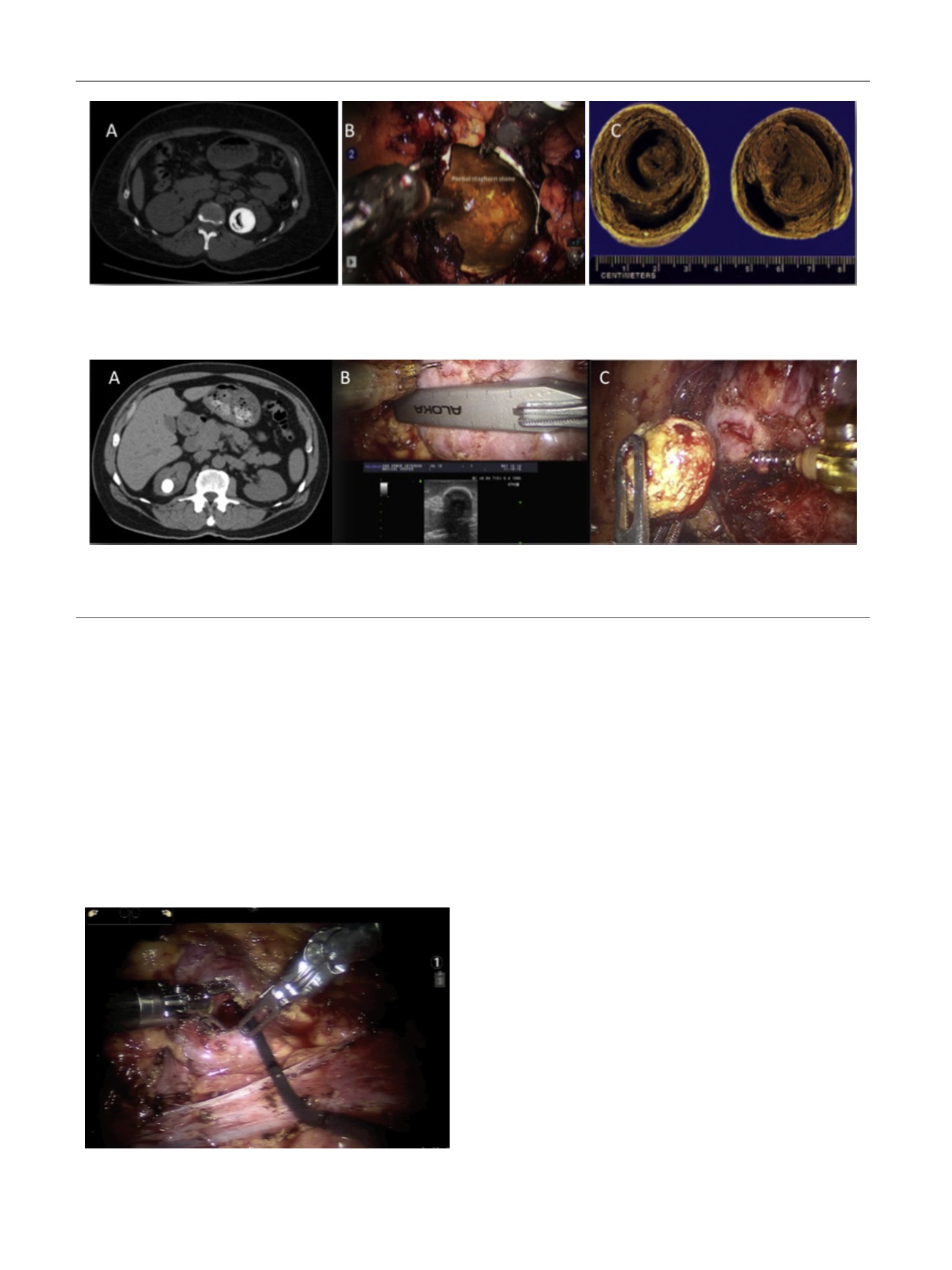
[(Fig._1)TD$FIG]
Fig. 1 – Robotic pyelolithotomy performed for a large pelvic stone. (A) Computed tomography scan demonstrating a 3.6-cm pelvic stone with possible
gas in the stone. (B) Pyelolithotomy incision exposing the stone. (C) Sectioned large left gas-containing renal stone.
[(Fig._2)TD$FIG]
Fig. 2 – Robotic nephrolithotomy performed for an upper pole stone. (A) A 2-cm upper stone within a diverticulum noted on computed tomography
scan. (B) A robotic ultrasound probe is utilized to identify and confirm the location of the stone and plan the incision. (C) A robotic ProGrasp forcep is
then used to carefully extract and remove the stone in its entirety.
[(Fig._3)TD$FIG]
Fig. 3 – Flexible nephroscopy being performed at the time of robotic
nephrolithotomy to inspect for residual stone.
E U R O P E A N U R O L O G Y 7 2 ( 2 0 1 7 ) 1 0 1 4 – 1 0 2 1
1016