















 990 1030
990 1030

relative to baseline values were 45% for IPSS and 67% for
Q
max
. This first clinical experience demonstrated that
implantation of TIND is a feasible and safe procedure, easy,
and fast to perform. Further studies are underway
(Clinicaltrials.gov: NCT02145208) to evaluate efficacy,
durability, and to define patient selection for this innovative
approach.
[16_TD$DIFF]
3.7.
PUL: Urolift
[17_TD$DIFF]
3.7.1.
Basic principle
The Urolift procedure (Neotract Inc., Pleasanton, CA, USA)
was officially approved by both the Food and Drug
Administration and National Institute for Health and Care
Excellence within 4 yr after first introduction
[41] .The
technical goal is to create a continuous anterior channel
through the prostatic lumen extending frombladder neck to
the verumontanum
( Fig. 2)
[42] .Tissue retracting implants
loaded on a dedicated delivery device are placed ante-
rolaterally at the 2 o’clock and 10 o’clock position under
cystoscopic control. On the one hand, preservation of the
neurovascular bundles and the dorsal venous plexus is
assured. On the other hand, encroaching lateral prostatic
lobes are compressed by the implants remodelling an open
anterior channel throughout the prostatic fossa. The
permanent Urolift implant is composed of a nitinol capsular
tab (diameter: 0.6 mm, length: 8 mm), an adjustable
polyethylene teraphtalate nonabsorbable monofilament
(diameter: 0.4 mm), and a stainless steel urethral end piece
(8 mm 1 mm 0.5 mm)
[41]. Unlike prostatic stents the
limited superficial exposure of the urethral end piece
minimises the risk of encrustation and after invagination
the implants are epithelialized. Usually, the implantation of
multiple retractors is required for successful treatment.
Patient selection is critical for optimal efficacy of the PUL
technique. Strict inclusion criteria were defined for
recruitment of patients in large RCTs in order to assess
efficacy in a particular subset of LUTS patients. Prostate
volumes between 20 cc and 70 cc with typical lateral lobe
obstruction (
kissing lobes
) are best addressed. More
challenging to treat are prostates larger than 100 cc or
patients with a high bladder neck or an obstructing middle
lobe and therefore, these anatomical features are consid-
ered (relative) contraindications. Notably, after PUL any
surgical interventions including TURP or laser-based
techniques are still possible without limitation. PUL can
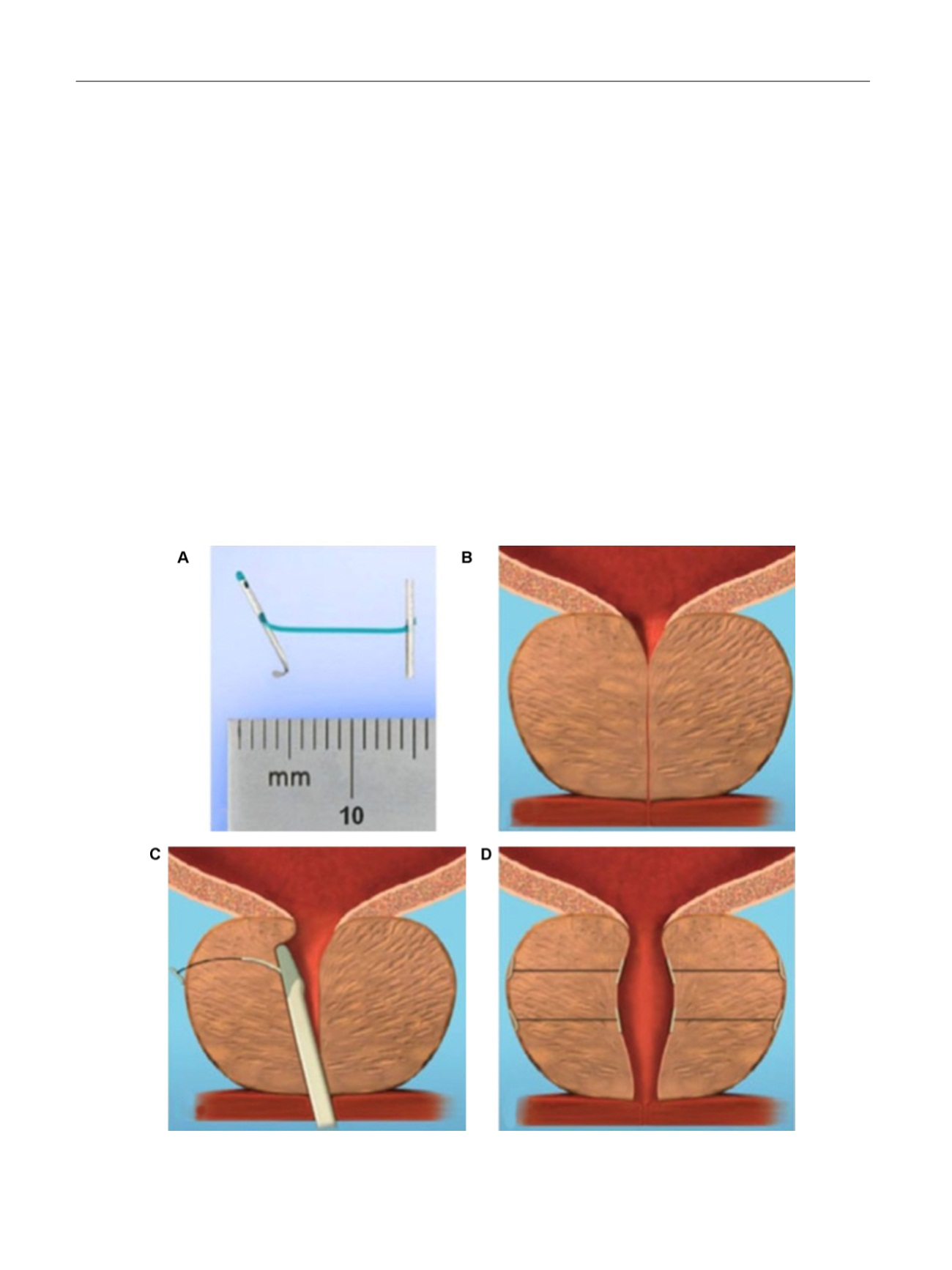
[(Fig._2)TD$FIG]
Fig. 2 – Prostatic urethral lift: Urolift. (A) Retracting implant composed of a nitinol capsular tab, a polyethylene terephthalate monofilament and a
stainless steel urethral end piece. (B) Benign prostatic obstruction by encroaching lateral lobes. (C) Delivery of retracting implant. (D) Expanded
urethra after compression of lateral lobes.
E U R O P E A N U R O L O G Y 7 2 ( 2 0 1 7 ) 9 8 6 – 9 9 7
990