















 932 1030
932 1030

1.
Introduction
Prostate cancer is the third leading cause of cancer death
among US men
[1] ;there are approximately 3.3 million
prostate cancer survivors, accounting for 21% of all cancer
survivors
[2].
Higher physical activity (PA) after diagnosis has consis-
tently been associated with a lower risk of dying from breast
cancer and colorectal cancer
[3–12] .Four large prospective
cohort studies suggest that postdiagnosis PA is also associated
with a lower risk of prostate cancer progression or prostate
cancer–specific mortality (PCSM)
[13–16]. However, the
strength of the evidence for PCSM is considered limited
due to concerns about reverse causation and limited power in
some of these studies
[15,16] .Therefore, a larger cohort study
with a design that minimizes bias from reverse causation is
needed. In addition, physical inactivity prior to diagnosis may
play a role in the development of tumor aggressiveness
[17] ,but this has not been well studied in relation to PCSM.
The goal of this study was to examine the associations of
pre- and postdiagnosis recreational PA with PCSM overall,
and by tumor risk category. The Cancer Prevention Study
(CPS)-II Nutrition Cohort is well suited for investigating
these associations, given its large sample size, long-term
follow-up, and detailed information on PA and important
covariates measured before and after diagnosis.
2.
Patients and methods
2.1.
Participants
Participants were drawn from the 86 402 men enrolled in the CPS-II
Nutrition Cohort, a prospective study of cancer incidence and mortality,
established by the American Cancer Society in 1992 as described in detail
elsewhere
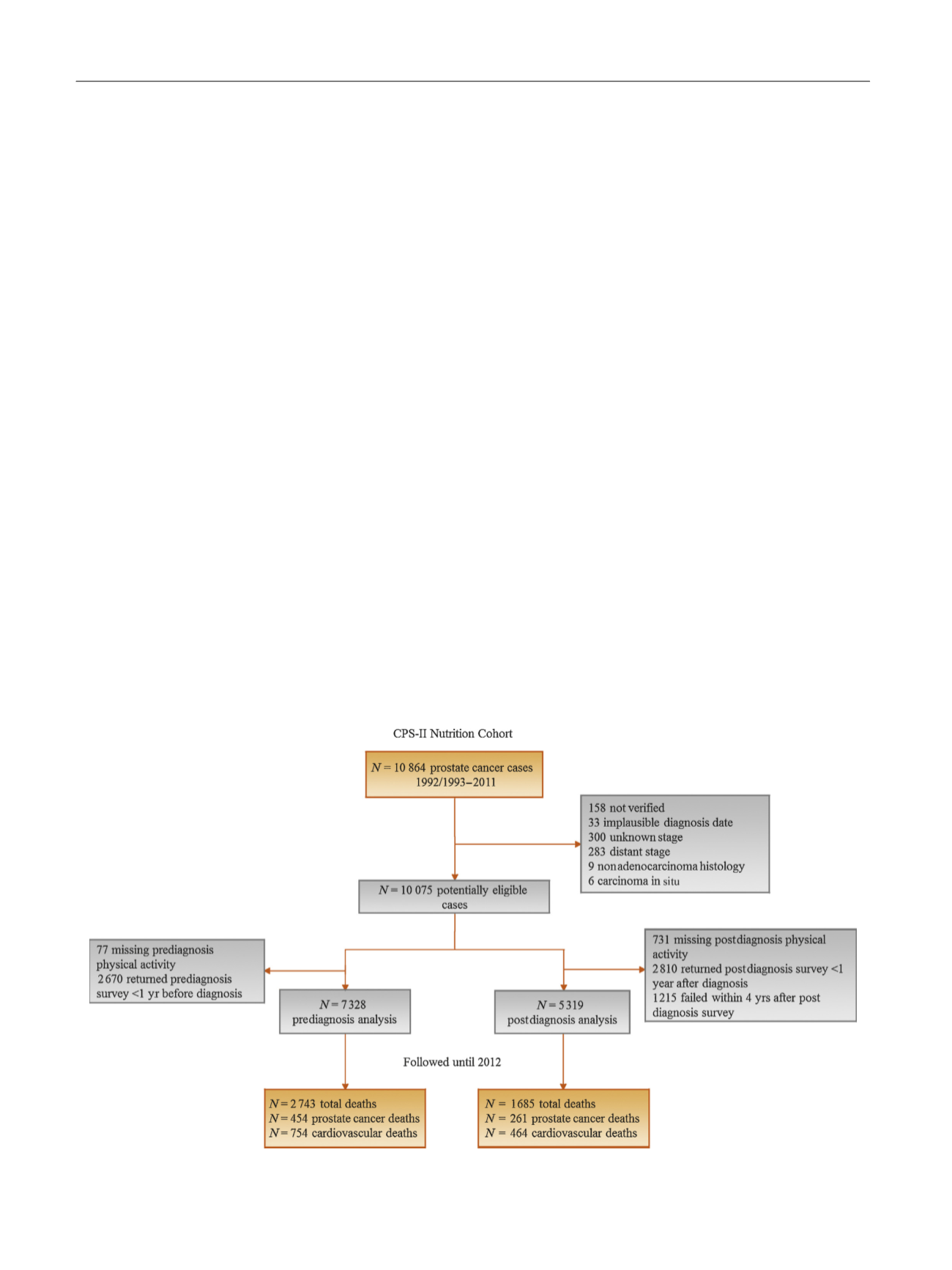
[18] .We identified 10 864 men diagnosed with prostate
cancer between 1992/1993 and June 30, 2011. After all exclusions
( Fig. 1 ), 7328 and 5319 men were included in pre- and postdiagnosis
analyses, respectively.
2.2.
Assessment of recreational PA
The amount of recreational PA per week during the past year was self-
reported on the baseline questionnaire and on biennial follow-up
questionnaires beginning in 1999 (except on the 2003 questionnaire;
available online:
https://www.cancer.org/research/we-conduct-cancer- research/epidemiology/cancer-prevention-questionnaires.html ). A meta-
bolic equivalent of task (MET) was assigned to each of the seven activities
as follows: 3.5 for walking, 3.5 for dancing, 4.0 for bicycling, 4.5 for aerobics,
6.0 for tennis or racquetball, 7.0 for jogging/running, and 7.0 for lap
swimming
[19]. Expert panels from organizations including the American
Cancer Society and American College of Sports Medicine recommend that
cancer survivors engage in a minimum of 150 min of moderate-intensity or
75 min of vigorous- intensity activity per week, or an equivalent
combination
[20,21]. Although strength training also is recommended for
cancer survivors, it was not asked on every questionnaire; thus, we focused
on aerobic exercise. We categorized the total recreational MET hours per
week (MET-h/wk) into four groups:
<
3.5, 3.5
<
8.75 (reference group),
8.75
<
17.5, and 17.5.Category 3.5
<
8.75 represents engaging in some
recreationalPA,equivalentto1–
<
2.5 hofwalkingperweek,butnotmeeting
the minimum recommendation. This reference group was selected because
it is larger than the lowest category, whichmeans that the risk estimates are
more stablewith narrower 95% confidence intervals (CIs), and is less subject
to reverse causation bias because men in the bottom category may have
reduced their activity due to illness.
Prediagnosis PA was obtained from the last questionnaire completed
at least 1 yr (median 3 yr) before prostate cancer diagnosis.
Postdiagnosis PA was obtained from the first questionnaire completed
at least 1 yr (median 3 yr) after diagnosis.
[(Fig._1)TD$FIG]
Fig. 1 – Prostate cancer cases drawn from the CPS-II Nutrition Cohort 1992/1993–2011, and number of deaths identified up to 2012. CPS = Cancer
Prevention Study.
E U R O P E A N U R O L O G Y 7 2 ( 2 0 1 7 ) 9 3 1 – 9 3 9
932