















 905 1030
905 1030

prostatectomy over AS
[17]. Our results expand upon this for
men who have already chosen conservative management,
showing that a high discount rate (focused on well-being in
the present) favors WW, while a low discount rate (places
more emphasis on future well-being) favors AS. This raises
the question as to whether time preferences should be
assessed as part of clinical decision-making; however, this
presents logistical challenges and would require further
research on how to perform such an assessment in clinical
practice.
As in all decision analyses, this study has several
limitations, including uncertainty for several model pa-
rameters. We performed extensive sensitivity analysis to
make this uncertainty transparent, revealing that few
parameters had a substantive impact on model results.
Notable exceptions are the extent and duration of QOL
impact from treatment-related complications, which vary
widely in the literature
[36] .That notwithstanding, our
model suggested that a switch in the preferred decision
would only occur with severe, lasting treatment-related
complications. Another drawback to our study is limited
published data for many AS testing strategies. However, the
model suggests that the precise protocol is not among the
key determinants of LYs or QALYs, confirming the robust-
ness of our results. Similarly, the amount of initial
misclassification may be lower using new genomic markers
and MRI-targeted biopsy. However, the results were robust,
and inferences for decision making changed neither in
sensitivity analyses with a hypothetical scenario of 0% initial
misclassification, nor in sensitivity analysis improving MRI
performance characteristics, suggesting that these are also
not key determinants of LYs or QALYs. Another limitation is
that we used a Markov cohort simulation, precluding the
ability to track test results over time. Follow-up studies
using microsimulation
[19]are warranted given that
reclassification is a conditional probability
[37]. Finally, in
order to compare the efficacy of different protocols under
ideal conditions, we assumed 100% compliance with
protocol-indicated biopsies and treatment recommenda-
tions when reclassification occurs. While we begin to
incorporate these data into patient counseling, future
studies are warranted, including an effectiveness analysis
with real-world adherence rates and incorporating other
end points such as cost effectiveness, which are also critical
for healthcare decision making
[38].
5.
Conclusions
AS extends life more than WW, but this is partly offset by
the decrement in QOL since a substantial proportion
ultimately undergo radical treatment. Patient preferences
had a significant influence on model results, and further
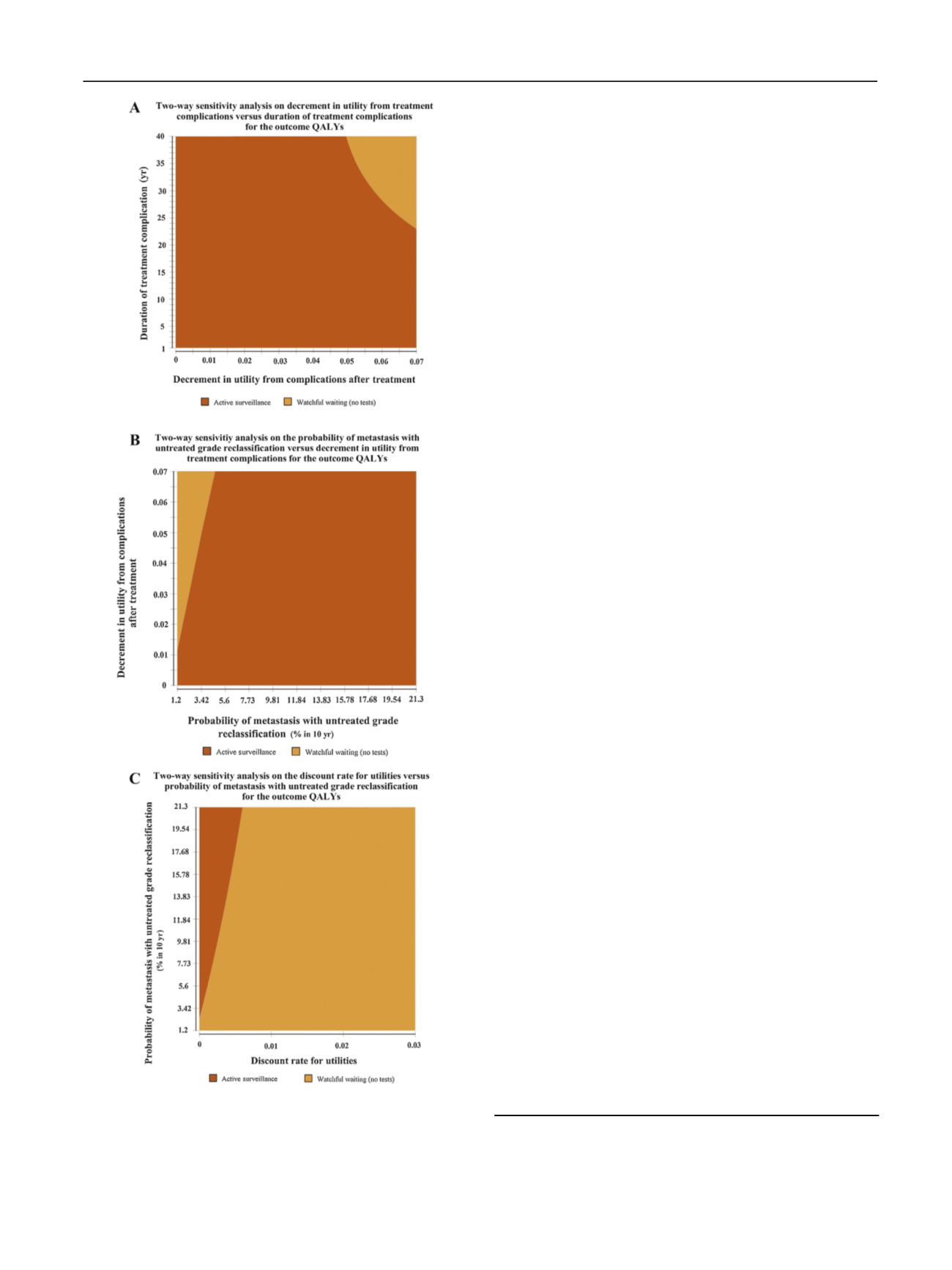
[(Fig._3)TD$FIG]
Fig. 3
–
Two-way sensitivity analyses for the (A) decrement in utility
from treatment complications and the duration of treatment-related
complications, (B) probability of metastasis for untreated grade
reclassification and decrement in utility from treatment-related
complications, and (C) discount rate and probability of metastasis with
untreated grade reclassification. Active surveillance (Hopkins) is
preferred with a shorter duration and less utility decrement from
treatment complications, and with an increasing probability of
metastasis for untreated grade reclassification, whereas watchful
waiting has more QALYs with a large decrement in utility and long
duration of treatment-related complications, and with a higher discount
rate. QALY = quality-adjusted life year.
E U R O P E A N U R O L O GY 7 2 ( 2 0 17 ) 8 9 9
–
9 0 7
905