















 866 1030
866 1030

Clinical studies show that in most clinical situations,
asymptomatic bacteriuria (ABU) has a low risk of progres-
sion to severe infection
[1]. The benefit of treating ABU with
antibiotics remains uncertain and requires clarification
with the need for better antibiotic stewardship
[2] .The aim of this systematic review was to synthesise
evidence about benefits and harms of treating ABU in
relevant patient groups. The review was undertaken as part
of the European Association of Urology (EAU) Urological
Infections Guideline 2017 update
[3]. Data extraction, risk
of bias (RoB) assessment using the Cochrane RoB Tool, and
quality assessment using the Grading of Recommendations,
Assessment,
Development and Education (GRADE)
approach
[4]were performed by two reviewers working
independently. The detailed methods and additional results
are described in the Supplementary material. Meta-
analyses were performed on data extracted from 50 pub-
lished trials recruiting 7088 patients (Supplementary
Table 1).
A single prospective, nonrandomised comparative study
investigated the effect of treating ABU in adult, nondiabetic,
nonpregnant women, and found no difference in the rate of
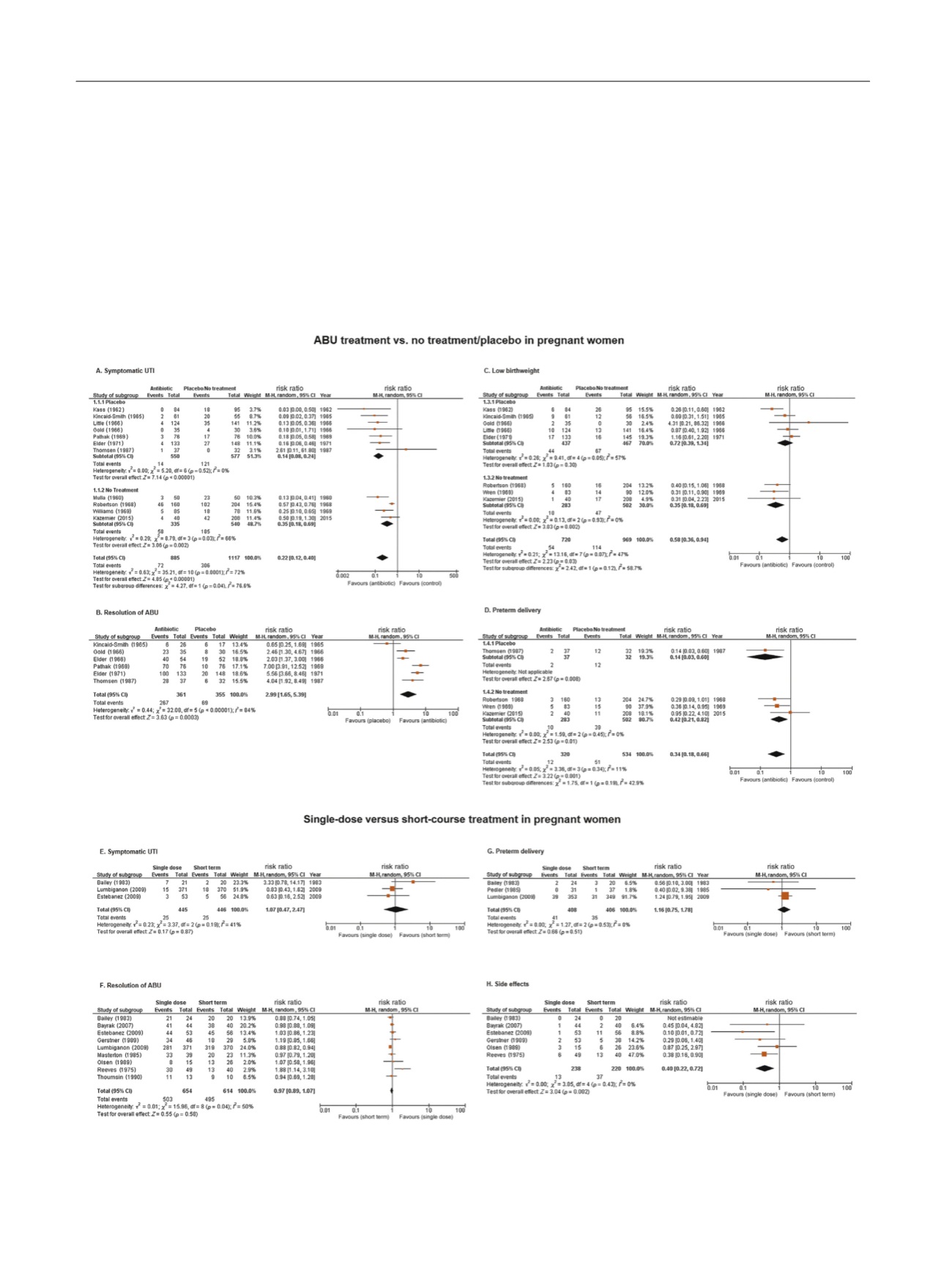
[(Fig._1)TD$FIG]
Fig. 1 – Forest plots on the effect of antibiotic treatment of ABU in pregnant women on (A) the rate of symptomatic UTI, (B) resolution of ABU, (C) rate
of low birthweight, and (D) rate of preterm delivery; a comparison of single-dose versus short-term antibiotic treatment of ABU in pregnant women
on (E) the rate of symptomatic UTI, (F) resolution of ABU, (G) rate of preterm delivery, and (H) rate of low birthweight. ABU = asymptomatic
bacteriuria; CI = confidence interval; M-H = Mantel–Haenszel; UTI = urinary tract infection.
E U R O P E A N U R O L O G Y 7 2 ( 2 0 1 7 ) 8 6 5 – 8 6 8
866